Foot Pain / Foot Drop
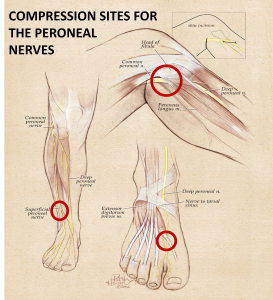
Foot Drop/Common Peroneal Nerves
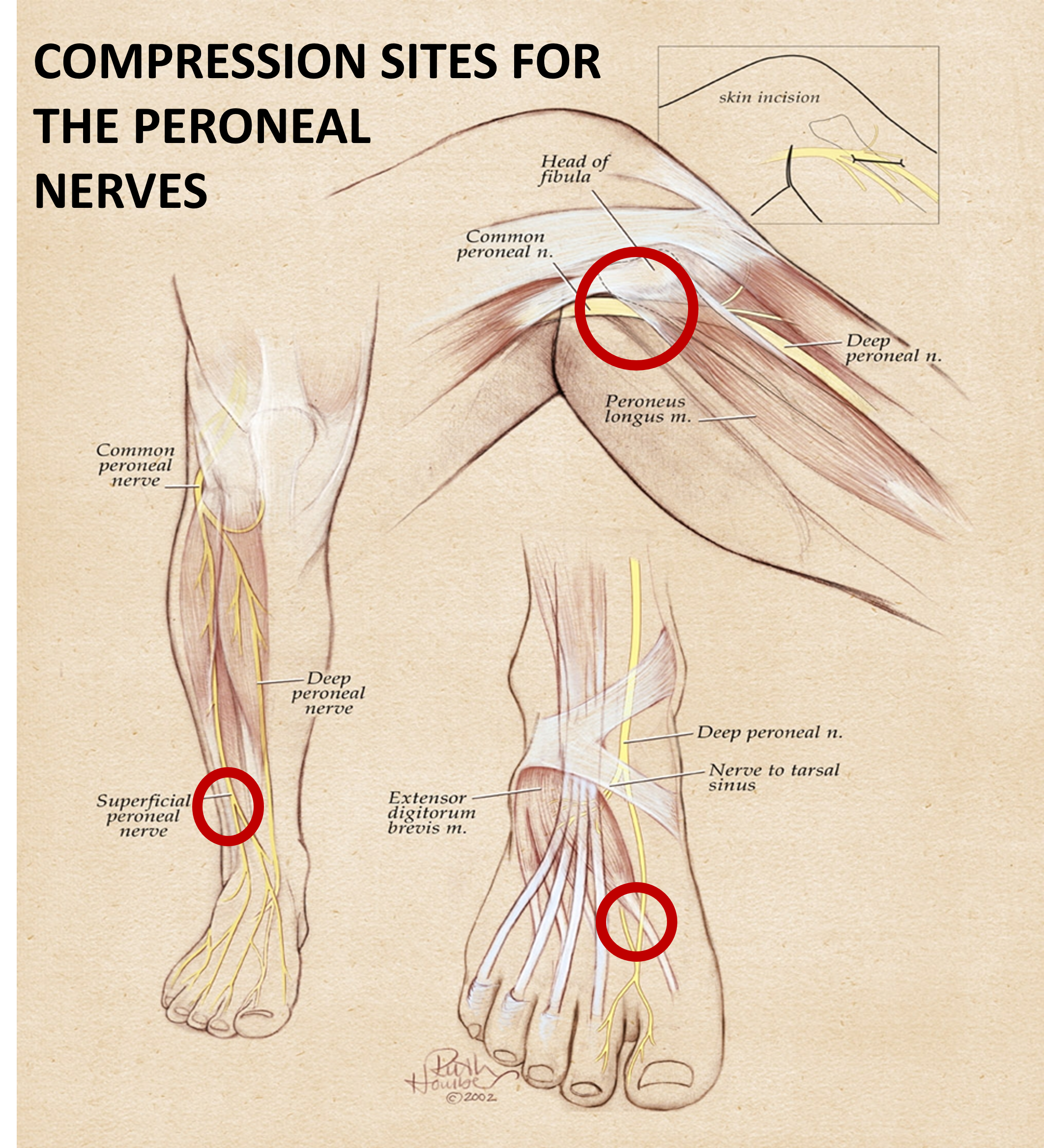
Common peroneal nerve dysfunction is damage to the peroneal nerve leading to loss of movement or sensation in the foot and leg.
Causes
The peroneal nerve is a branch of the sciatic nerve, which supplies movement and sensation to the lower leg, foot and toes. Common peroneal nerve dysfunction is a type of peripheral neuropathy (damage to nerves outside the brain or spinal cord). This condition can affect people of any age.
Dysfunction of a single nerve, such as the common peroneal nerve, is called a mononeuropathy. Mononeuropathy means the nerve damage occurred in one area. However, certain body-wide conditions may also cause single nerve injuries.
Damage to the nerve destroys the myelin sheath that covers the axon (branch of the nerve cell). Or it may destroy the whole nerve cell. There is a loss of feeling, muscle control, muscle tone, and eventual loss of muscle mass because the nerves aren’t stimulating the muscles.
- Trauma or injury to the
 knee
knee - Fracture of the fibula (a bone of the lower leg)
- Use of a tight plaster cast (or other long-term constriction) of the lower leg
- Crossing the legs regularly
- Regularly wearing high boots
- Pressure to the knee from positions during deep sleep or coma
- Injury during knee surgery or from being placed in an awkward position during anesthesia
- Who are very thin (for example, from anorexia nervosa)
- Who have conditions such as diabetic neuropathy or polyarteritis nodosa
- Who are exposed to certain toxins that can damage the common peroneal nerve
Symptoms
- Decreased sensation, numbness, or tingling in the top of the foot or the outer part of the upper or lower leg
- Foot that drops (unable to hold the foot up)
- “Slapping” gait (walking pattern in which each step makes a slapping noise)
- Toes drag while walking
- Walking problems
- Weakness of the ankles or feet
Exams and Tests
- Loss of muscle control in the lower legs and feet
- Atrophy of the foot or foreleg muscles
- Difficulty lifting up the foot and toes and making toe-out movements
Tests of nerve activity include
- Electromyography (EMG, a test of electrical activity in muscles)
- Nerve conduction tests
- MRI
- Nerve ultrasound
What other tests are done depend on the suspected cause of nerve dysfunction, and the person’s symptoms and how they developed. Tests may include blood tests, x-rays and scans.
Treatment
Treatment aims to improve mobility and independence. Any illness or other cause of the neuropathy should be treated. Padding the knee may prevent further injury by crossing the legs and remind you to not cross your legs.
Corticosteroids injected into the area may reduce swelling and pressure on the nerve in some cases.
You may need surgery if:
- The disorder does not go away
- You have problems with movement
- There is evidence that the nerve axon is damaged
Surgery to relieve pressure on the nerve may reduce symptoms if the disorder is caused by pressure on the nerve. Surgery to remove tumors on the nerve may also help.
CONTROLLING SYMPTOMS
You may need over-the-counter or prescription pain relievers to control pain. Other medications may be used to reduce pain include gabapentin, carbamazepine, or tricyclic antidepressants such as amitriptyline. Whenever possible, avoid or limit the use of medication to reduce the risk of side effects.
If your pain is severe, a pain specialist can help you explore all options for pain relief.
Outlook (Prognosis)
The outcome depends on the cause of the problem. Successfully treating the cause may relieve the dysfunction, although it may take several months for the nerve to grow back.
However, if nerve damage is severe, disability may be permanent. The nerve pain may be very uncomfortable. This disorder does NOT usually shorten a person’s expected lifespan.
Possible Complications
- Decreased ability to walk
- Permanent decrease in sensation in the legs or feet
- Permanent weakness or paralysis in the legs or feet
- Side effects of medication
When to Contact a Medical Professional
Call your health care provider if you have symptoms of common peroneal nerve dysfunction.
Prevention
Avoid putting long-term pressure on the back or side of the knee. Treat injuries to the leg or knee right away.
Alternative Names
Neuropathy – common peroneal nerve; Peroneal nerve injury; Peroneal nerve palsy
References
King JC. Peroneal neuropathy. In: Frontera WR, Silver JK, Rizzo TD, eds. Essentials of Physical Medicine and Rehabilitation: Musculoskeletal disorders, pain and rehabilitation. 2nd ed. Philadelphia, Pa: Saunders Elsevier; 2008:chap 66.
Update Date: 9/25/2013
Updated by: Joseph V. Campellone, MD, Department of Neurology, Cooper University Hospital, Camden, NJ. Review provided by VeriMed Healthcare Network. Also reviewed by David Zieve, MD, MHA, Bethanne Black, and the A.D.A.M. Editorial team.